
 Share on Facebook
Share on Facebook
 Share on Twitter
Share on Twitter
 Share on LinkedIn
Share on LinkedIn
 Share by Email
Share by Email
 Print
Print

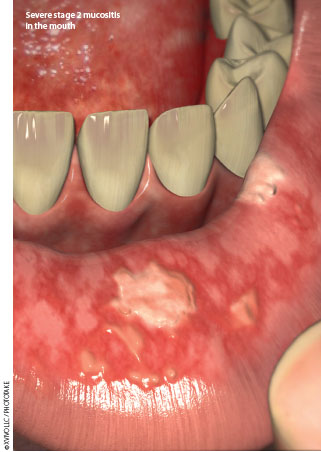
Each year, 132,000 oncology patients in the United States (2003 data)1 develop oral mucositis, one of the most frequent and distressing side effects of cancer treatment.1-5 Oral mucositis refers to inflammation of the oral mucosa that in severe cases may lead to ulceration and causes a disruption in the function and integrity of the mouth resulting from cancer therapy.6-8 Forty percent of all patients undergoing chemotherapy and/or radiation therapy will experience this side effect.2,3,9-11 Oral mucositis poses great danger to patients and also negatively impacts the health care delivery system. Besides increasing the patient’s risk of local or systemic infections,8,11,12 oral mucositis can raise the cost of health care by at least $1,700 per patient, depending on severity.9,13-15
What are effective strategies to prevent oral mucositis? What type of education do patients and families need to avoid this troublesome side effect or to at least make it more manageable? Existing evidence demonstrates that clinicians have limited knowledge of evidence-based oral care16-18 and that nurses’ skill with oral care needs improvement.18 The development of a specific policy regarding oral care for oncology patients may help, as one evidence-based practice team found.
DEVELOPING AN EVIDENCE-BASED POLICY
 The Oral Mucositis Committee, a multidisciplinary team formed at a large academic medical center (the University of Iowa Hospitals and Clinics and the University of Iowa Children’s Hospital), sought to develop an evidence-based oral care policy to address oral mucositis and promote oral health for oncology patients. Team members represented adult and pediatric areas, inpatient and ambulatory care settings, oncology and bone marrow transplant, nursing, medicine, dietary, speech and swallowing services, dentistry, and pharmacy.
The Oral Mucositis Committee, a multidisciplinary team formed at a large academic medical center (the University of Iowa Hospitals and Clinics and the University of Iowa Children’s Hospital), sought to develop an evidence-based oral care policy to address oral mucositis and promote oral health for oncology patients. Team members represented adult and pediatric areas, inpatient and ambulatory care settings, oncology and bone marrow transplant, nursing, medicine, dietary, speech and swallowing services, dentistry, and pharmacy.
An evidence-based practice model was used to guide implementation of the recommended changes, which included developing a policy, educating nursing and medical staff, creating outreach strategies, modifying the computerized documentation system, and providing audit and feedback after implementation.19
Evaluating the patient One of the first and often overlooked things to evaluate is the current oral care practices of the patient, family, and/or caregiver and any associated barriers to good oral health that may exist. For some patients, oral care may only include brushing their teeth once a day or every other day, whereas for others, oral care might mean brushing twice a day and flossing once a day. Variability among patients’ baseline oral care practices means that nurses need to critically think about how to best individualize patient education while highlighting the same educational concepts for each patient. Education must include the importance of good oral care, frequency of oral care, correct technique, and the appropriate use of certain oral care products in order to remove food debris and plaque. Education should also focus on encouraging patients to stop smoking and/or using chewing tobacco, if applicable and age-appropriate. Good oral care decreases the risk of oral mucositis and systemic infection.20-22
Contraindications Nurses must also consider any contraindications to routine oral care. For example, oral care may be inappropriate or require special considerations for patients recovering from oral surgery to avoid trauma to the surgical site. Additionally, patients at risk to aspirate should be carefully considered, as they have an elevated risk of aspiration pneumonia if oral care is poor.23 The policy developed by the Oral Mucositis Committee did not address mechanically ventilated patients or those with tracheotomies but did provide nurses with a link to the appropriate policy for these patient populations.

